肺部SBRT的螺旋断层治疗临床方案和试验
时间:2023-01-15 12:01:35 热度:37.1℃ 作者:网络
TomoTherapy系统是最早提供图像引导放射治疗(IGRT)体积图像的临床系统之一。尽管软组织的MVCT图像对比度较差,但这些图像足以根据骨骼解剖结构为患者定位 【1】。对于肺癌患者来说,肿瘤和肺实质之间的巨大反差使肿瘤可以直接定位。这对肺部肿瘤来说非常重要,因为肺部肿瘤相对于骨骼通常会移动。即使是亚厘米大小的肺部小肿瘤,MVCT也能提供有用的可视化效果,使患者精确定位(图1)。这种大小的肿瘤很难在二维成像中显示出来,而在CT用于图像引导放射治疗之前,二维成像技术就已经在使用了。与早期提供IGRT的其他竞争平台相比,TomoTherapy的IGRT工作流程整合良好,非常适合肺SBRT 治疗。一项研究统计了8名接受3~5个SBRT分割治疗的患者,显示MVCT可以达到亚毫米精度【2】。因此,当计划靶区中包含足够的几何外扩时,TomoTherapy可以准确地将高分次剂量投照给一个高活动性的小肿瘤。治疗结果如图2所示;治疗后3个月,肿瘤体积明显缩小;治疗后6个月,以原发肿瘤部位为中心,肺组织形成的球形磨玻璃实变形态,显示治疗的准确性。

图1 基于MVCT和 kVCT配准的肺 SBRT患者摆位。肺部肿瘤直径为9mm。
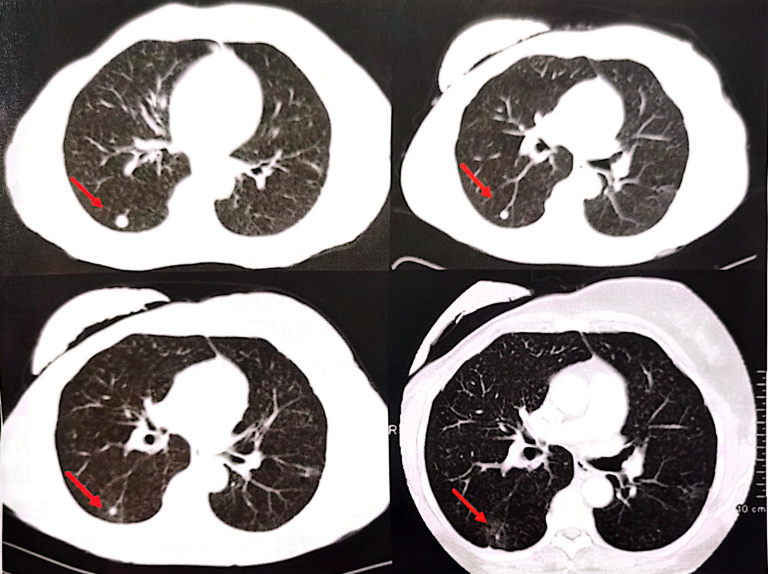
图2 治疗结果随访CT显示肿瘤退缩以及治疗后肺部肿瘤周围球状毛玻璃肺组织的改变。
这些图像显示的是治疗前和治疗后2个月、3个月和6个月的CT。
由于IGRT方案成熟,且调强放疗计划系统相对于同期的系统较为先进,所以在最初商业化使用的几年中,TomoTherapy就得到了广泛的普及和临床应用。与此同时,与差强人意的常规分次剂量递增研究相比,肺部SBRT已经成为不可手术的早期非小细胞肺癌(NSCLC)患者的一种值得期待的治疗方式。威斯康辛大学首次证明了,应用螺旋断层治疗实施肺SBRT的可行性,整个过程没有出现重大技术限制或急性毒性【3】。Dunlap 等人报道使用螺旋断层治疗早期NSCLC有很好的局部控制【4】。Aibe报道了螺旋断层治疗对早期肺癌患者具有良好的局部控制和生存率【5】,GTV尺寸依赖的严重毒性率很低(6.7%)。最近,Nagai 等人证明了通过螺旋断层治疗实施肺SBRT是安全有效的【6】。对于多发性肺转移的患者,Kim表示,螺旋断层治疗提供了安全有效的局部控制【7】。肺SBRT的一个主要问题是,当肿瘤的位置靠近中枢器官时,对正常器官的毒性需要格外关注【8-12】。使用螺旋断层治疗可以在肿瘤及其邻近的中枢器官之间创造一个陡峭的剂量梯度【13】,从而能够降低严重毒性的风险。
参考文献:
[1]Boswell,S.et al.,Automatic registration of megavoltage to kilovoltage CT images in helical tomothcrapy:An evaluation of the setup verification process forthe special case of a rigid head phantom. Med Phys, 2006.33(11):4395-404.
[2]Zhou,J.N. et al.,Imagc-guided stereotactic brxdy radiotherapy for lung tumors using Bodyloc with tomo-therapy: Clinical implementation and set-up accuracy. Med Dosim,2010.35(1):12-8.
[3]Hodge,W,et al.,Feasibility report of image guided stereotactic body radiotherapy(IG-SBRT)with to-
motherapy for early stage medically inopcrable lung cancer using extreme hypofractionation. Acta Oncol, 2006.45(7):890-6.
[4]Dunlap,N.E.ct al.,Size matters:A comparison of Tl and T2 peripheral non-small-cell lung cancers
treated with stercotactic body radiation therapy(SBRT).J Thorac Cardiovasc Surg.2010.140(3):583-9.
[5]Aibe,N. et al.,Outcome and toxicity of stereotactic body radiotherapy with helical tomotherapy for inoper-able lung tumor: Analysis of Grade 5 radiation pneumonitis.J Radiat Res,2014.55(3):575-82.Epub 2014/01/25.
[6]Nagai,A.et al.,Safety and efficacy of intensity-modulated stereotactic body radiotherapy using helical to-motherapy for lung cancer and lung metastasis.Biomed Res Int,2014.2014:473173.
[7]Kim,J.Y.et al.,Helical tomotherapy for simultaneous multitarget radiotherapy for pulmonary metastasis.Int J Radiat Oncol Biol Phys,2009.75(3):703-10.Epub 2009/05/08.doi:10.1016/j.jrobp.2008.11. 065;S0360-3016(09)00196-5[pii].PubMed PMID:19419818.
[8]Rowe,B.P.et al.,Stereotactic body radiotherapy for central lung tumors.J Thorac Oncol,2012.7(9):
1394-9.
[9]Haasbeek,C.J.et al.,Outcomes of stereotacticablative radiotherapy for centrally located early -stage lung cancer.J Thorac Oncol,2011.6(12):2036-43.Epub 2011/09/06.
[10] Song,S.Y. ct al.,Fractionated stereotactic body radiation therapy for medically inoperable stage I lung cancer adjacent to central large bronchus.Lung Cancer,2009.6(1):89-93.
[11]Joyner,M. et al.,Stereotactic body radiation therapy for centrally located lung lesions. Acta Oncologica,2006.45(7):802-7.
[12]Timmerman,R. et al.,Excessive toxicity whentreating central tumors in a phase ll study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer.J Clin Oncol,2006.24(30):4833 -9.
[13] Chi,A. et al.,Feasibility of helical tomotherapyin stereotactic body radiation therapy for centrally located early stage nonsmall-cell lung cancer or lung metastases.Int J Radiat Oncol Biol Phys,2011.81(3):856 -62.
: , 。 视频 小程序 赞 ,轻点两下取消赞 在看 ,轻点两下取消在看

